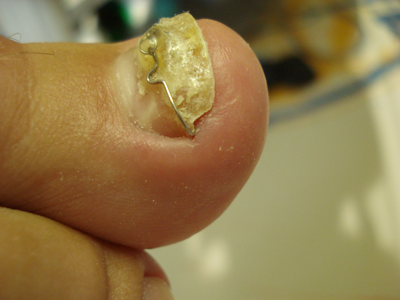
Ingrown nail is a painful inflammatory condition caused by a nail edge that has usually been rendered sharp by improper trimming because embedded spurs remain.
Ingrown Toenail with Recovered Embedded Spur
Ingrown toe-nail is a reIatively common Iesion that is most prevaIent amongst young aduIts with a greater number in men. Whereas only 0.02% of the general population develop ingrown toenails, Dardignac who had 6000 infantry men under his care observed 2%.
Ingrown toenails also called onychocryptosis, are characterized by pain when walking and on touch with signs of inflammation in the nail fold. It may develop on normal looking toe, almost exclusively on the great toe of either foot. The almost exclusive occurrence of ingrown toenails on the great toe is probabIy due to the prominence of that toe on the foot, the relativeIy wide naiIwaIIs, and the great use of this toe in waIking.
The skin around the nail is punctured by the nail plate resulting in foreign body stimulation, inflammation, infections, and reparative processes with soft tissue hypertrophy of the skin in the nail fold. Reduced physical activity is thought to be a general risk factor of ingrown toenails. Pressure applied to the sole of the toes by walking maintains the shape of the nails and prevents them from rolling up.
Under normal conditions, the upward mechanical force and the constitutive nail shrinkage force are well-balanced. However, in some people, the constitutive nail shrinkage force may exceed the upward mechanical force, either because the patient lacks sufficient mechanical forces on the nail due to being bedridden or wearing ill-fitting shoes that do not allow sufficient pressure on the first toe on walking or because the constitutive nail shrinkage force is excessive due to genetic or systemic disease influences. Inappropriate nail cutting further promotes nail overcurvature according to Sano et al. (2015).
Genetic predisposition may result in an excessive automatic shrinkage force that causes the nail to curve inward and stick into the lateral soft tissue, which leads to pain. However, when the patient seeks to reduce the pain and cuts away the sore corners of the nails then nail overcurvature is further promoted. The vicious circle leads to further overcurvature of the nail by reducing the upward mechanical force on the first toe by altering the gait, reducing ambulation, and wearing ill-fitting shoes, that do not exert sufficient pressure on the first toe.
The nail apparatus consists of the nail plate, the nail fold, the nail matrix, the sterile matrix and the hyponychium.
The nail plate is a durable layered keratinized structure that is formed continuously with dorsal, intermediate, and ventral nail plates. It arises from the maturation and keratinization of the nail matrix and is firmly connected to the sterile matrix. The dorsal and intermediate layers of the nail plate are produced by the nail matrix, whereas the ventral layer is produced by the sterile matrix.
The sides of the nail plate are bounded by lateral nail folds that are related to the proximal fold. The lateral nail folds are cutaneous folded structures that enclose the lateral free edges of the nail plate providing the lateral borders to the nail.
The proximal ( posterior ) nail fold is a skin fold that provides the visible proximal border of the nail. On the lower portion of the undersurface, this becomes the dorsal matrix. The Eponychium refers to the upper portion of the ventral aspect of the proximal of nail fold. The cuticle is the tissue that seals the nail cul-de-sac which is formed by the dorsal and ventral side of the proximal nail fold.
The nail matrix (nail root) is a specialized epithelial structure that overlies the central portion of the distal phalanx. Keratinocytes of the nail matrix divide in the basal cell layer and keratinize above. The distal matrix is partially covered by the proximal nail fold. The convex margin of the matrix is visible through the nail plate as a white crescent-shaped area more pale than the adjacent nail bed called the lunula (half moon).
The sterile matrix epidermis, the nail bed, the vascular bed upon which the nail rests extends from the distal edge of the lunula to the hyponychium. Sterile matrix cells differentiate into the nail plate. The contribution of the sterile matrix to nail plate formation is approximately one fifth the thickness and mass of the terminal nail.
The hyponychium is the cutaneous margin under the free nail between the onychodermal band and the distal grove. The onychodermal band creates a grey line at the edge of the nail bed before the free edge of the nail plate. It represents the first barrier to penetration of materials to beneath the nail plate. The distal grove (limiting furrow) is an epidermal ridge demarcating the border between subungual structures and the toe pad.
Toenails protect the distal toes. However, they are always exposed to physical stimulation such as counter pressure and shear force. These mechanical forces may have a pronounced effect on nail configuration.
Nails are actually equipped with an automatic curvature force that helps them to adapt to daily upward mechanical forces. When the upward mechanical and the automatic curvature forces are well balanced, the configuration of the nail is normal.
Therefore, pincer nails may be caused by a lack of upward mechanical forces that occur when standing and walking. Evidence for this is provided by a study of Sano H. & Ichioka S. who found that there is a high incidence of pincer nail among bedridden patients whose feet are not used for walking. Further evidence for this effect of the lack of upward force is that the degree of great toe nail curvature in the patients of that study tended to increase as the duration of the bedridden state rose.
As outlined above nail plates are composed of a layered structure, namely, dorsal, intermediate, and ventral layers. The dorsal and intermediate layers of the nail plate are produced by the nail matrix, whereas the ventral layer is produced by the sterile matrix. The sterile matrix contains mechanoreceptors through which mechanical forces such as standing and walking promote cell proliferation and differentiation. The lack of mechanical stimuli in bedridden patients may result in pincer nail formation through a mismatch in growth of the matrix-oriented dorsal and the sterile matrix-oriented ventral layer. In fact pincer nails show a greater inward curvature on the distal side as a result of shortening of the ventral layer.
The term pincer nail was introduced by Cornelius and Shellery in 1968 and is defined as the transverse overcurvature of the nail plate that increases along the longitudinal axis with an unusual degree of thickness producing a pathologic degree of pinching of underlying soft tissue under the affected nail with severe pain in the involved toe. Ingrown nails resemble pincer nails as they are characterized by a sharp irregular nail edge that involves the distal corners of the nails.
When the sharp nail corner is cut off, the increase in overcurvature is facilitated. Thus at the clinical level ingrown nail associate with pincer nail. The term ingrown nail describes the growth of the nail into the flesh whereas pincer nail describes the appearance of the nail.
Risk factors for pincer nail and ingrown nail include heredity, toe trauma, inappropriate nail cutting, obesity, lower activity levels and in particular, the physical forces caused by ill-fitting shoes. High heels of the shoes increase the pressure on the toes. Women’s shoes are usually narrow in the toe area. This increases the pressure under the fifth metatarsal head and leads to callous formation, as the study by Ryutaro Kase et al. has shown.
As mentioned above there is also a high incidence of pincer nail among bedridden patients whose feet are not subjected to shoes or weight bearing. Also in children with hematologic malignancies and solid tumors during chemotherapy and stem cell transplantation the incidence of ingrown toenails is high, namely 13%.
The indications for treatment of pincer nails and ingrown nails are pain, inflammation, interference with wearing shoes, and cosmetic embarrassment.
Conservative procedures are usually employed first. The conservative treatments involve the use of an elastic wire or a plastic device and aim to reinforce the upward daily mechanical force.
An effective conservative treatment method to handle stage 1 of ingrown toenails is soaking in warm water, elevation of nail corner with a cotton packing and avoiding ill-fitting footwear that is either too tight or too lose.
If the nail corner is of sufficient Iength, a smaIl pIedget of cotton moistened with aIcohol is inserted gently between the edge of the nail and the soft parts, in such a way as to aIIow some of the cotton to extend sIightIy under and above the nail edge. This is best done by puIIing the soft parts away from the nail, so as to expose the edge.
Sometimes, however, when the patient is first seen, the corners are cut so short that it is impossible for the cotton to be inserted and retained. The patient is then instructed to soak and cleanse his foot in a warm water bath for an hour twice a day, and to wear white socks that are changed daily.
The patient is then instructed to wear suitable shoes and shown how to properly trim the toenails so that they have a straight free edge. When cutting down the side of the nails to make the edges round, it is easy to overlook nail residues, which then grow in in the depth of the nail fold.
Improper Trimmed Nail - Corners Cut
Surgery for Ingrown Toenails
Winograd Procedure or Emmert Plasty
How is the problem portion of an ingrown toenail surgically removed?
Among the various surgical treatments for ingrown toenails, the modified Winograd method and the Emmert Plasty are the most widely used operative modalities for ingrown toenails.
The procedure begins with the placement of a constricting band around the toe to reduce blood flow and the administration of local anesthetic to numb the toe.
An incision splits the ingrown edge of the toenail from the rest of the nail and continues down through the tissue beneath the nail to the surface of the bone.A second incision is carried out down through the overlapping tissue on the outer edge of the nail. This wedge of nail including it’s root and tissue is freed and removed from the toe resulting in a slightly thinner toenail.
The operative site is closed with sutures. The constricting band is removed, and the toe is bandaged and wrapped. Surgical removal of an ingrown toenail results in a narrower nail width.
Toe nail following surgery with narrower width
Clinical Study Comparing Nail Bracing with Surgery
Treatment of Ingrown Toenails Using
a New Conservative Method
The first prospective study to directly compare an orthonyxia technique with a standard operative procedure for the treatment of an ingrown toenail was the study by Harrer et al. published in 2005. They compared a conservative method employing the VHO-Ost-hold brace ( VHO-Osthold-Spange GmbH, Deisenhofen, Germany ) with Emmert’s ( Winograd’s ) surgical procedure in 41 patients with a symptomatic ingrown toenail of the great toe.
They found that pain caused by treatment with the brace was significantly lower than that recorded for postoperative pain in the Emmert’s surgical procedure group. Furthermore, most of the patients in the brace group reported an appreciable reduction in pain after placement of the device. After initial treatment, patients in the brace group could wear regular shoes again without experiencing severe pain significantly earlier than patients undergoing Emmert’s surgical procedure.
The average duration of treatment was shorter in the Emmert surgical procedure group. However, none of the patients in the brace group had to take time off from work, whereas in the Emmert procedure group, working patients were off from work for an average of 14.7 days. Therefore the estimated total cost to the economy in the case of working patients was US $1,975.20 in the Emmert surgical procedure group and approximately US $334.30 in the brace group with equal outcome in terms of recurrences for the two groups.
A Big Toe Nail after 3 Operations
Efficacy of Nail Braces for Acute and Chronic Ingrown Toenails
In this prospective study Wang et al. treated 53 patients with ingrown toenails. The ingrown toenails were classified into 2 clinical types, acute inflamed and dystrophic–type. Chronic dystrophic–type ingrown toenails manifested as dystrophic nails with nail bed atrophy and lateral nail fold hypertrophy but without obvious inflammation. The nail plate was usually hard, atrophic, thickened, and/or C-curved and the nail bed atrophic.
Using the Heifetz classification 11 sides (31.4%) had Stage I, 9 (25.7%) had Stage II, and 15 (42.9%) had Stage III ingrown toenails among the acute inflamed-type group. Two types of braces were used in this study. Brace 1 was composed of an adhesive pad with an embedded activating wire, whereas brace 2 was made up of a spring-wired hook and a square adhesive pad. The hook was attached to the rim of the nail plate, and the pad was glued onto its dorsum.
Pain relief was achieved in almost all patients within 1 day, and they were able to return to work immediately. Chronic dystrophic-type ingrown toenails required longer treatment duration to achieve excellent results than acute inflamed-type ingrown toenails. Recurrence rate was 4 % in chronic dystrophic-type ingrown toenails and 13 % in acute inflamed-type ingrown toenails.
Nail Brace Application in Diabetic Patients with Ingrown Nails
Since ingrown toenails are one of the skin lesions considered as a risk factor for diabetic foot disease adequate management of ingrown toe nails is especially crucial in patients with diabetes mellitus since the prevalence of ingrown toe nails is greater in patients with diabetes mellitus than in the healthy population. Body mass index,previous trauma, a weak dorsalis pedis pulse, nail trimming type, onychogryphosis, and subungual hyperkeratosis are predictive variables for ingrown toe nails in adult diabetic patients according to a study published 2018 by Secil Vural et al. in the Journal of Foot and Ankle Surgery.
In the study of Erdogan & Erdogan for the treatment of ingrown toe nails in diabetic patients a simple nail device without any systemic treatment or surgical intervention was investigated in 21 diabetic patients who all had severe pain, erythema, and edema without suppuration or granulation tissue formation. However, all patients had immediate relief of symptoms once the nail brace was applied. Stopping the irritation in the nail fold by nail brace treatment might also help prevention of infection in diabetics.
Nail braces were applied until all the symptoms were cleared. The patients were followed for 2 years for the recurrence of symptoms and signs. 15 of 21 patients did not have any recurrences for 2 years. The 6 patients who had recurrence of painful ingrown nails were willing to get the nail brace once more instead of having a surgical procedure.
Therefore, nail brace application is a safe, simple, and inexpensive treatment option for diabetic patients with ingrown toe nails. In case of a recurrence, patients are willing to have it for a second time as it is simple and painless treatment.
Nail brace application for ingrown nails in children.
An ingrown toenail causes a child to have tenderness, redness, and swelling of the skin around the corner of the toenail on one of the big toes. Shih et al. in their study reported on 38 children between 6 and 17 years of whom 60% had stage III and 26% stage II ingrown toenails. Nail brace application was tolerated well by all children without local anesthesia.
Nail brace treatment of ingrown toe nails in children rapidly relieved symptoms, had a short return-to-daily-activity time, and led to high patient satisfaction. A recurrence was noted in 8 patients (21%).
Summary of Clinical Studies on Brace Treatment for ingrown toenails.
The studies presented show that the outcome of bracing of ingrown toenails in terms of recurrences is equal to a surgical procedure. However, following a surgical procedure patients were off work for a fortnight.
Nail bracing is possible in acute inflamed type and chronic dystrophic-type ingrown toenails with higher recurrence rates in the inflamed type group of patients. However, chronic dystrophic-type ingrown toenails require longer treatment times to achieve excellent results.
Furthermore it has been shown that nail bracing is also a safe, simple, inexpensive and treatment option for diabetic patients with ingrown toe nails. Finally it was demonstrated that nail bracing is also a viable option for children with ingrown toenails.
Nail Braces used for the Treatment for ingrown toenails in Clinical studies.
In general, the spring wire of nail braces gently lifts the sides of the toenail and gradually forces the nail to grow to a flatter shape over time.
Harrer et al. in their study 2005 in Erlangen, Germany, employed the so called VHO-Osthold Nail Brace which was invented by podiatrist Elvira Osthold. The VHO-Osthhold nail brace consists of 3 parts that are made of surgical spring steel wire with 2 legs hooked on the sides of the nail and the 3rd part, a loop wire that ties the 2 legs thus exerting tension on the side walls of the nail so that the nail fold is immediately relieved.
In the study by Wang et al. the so called COMBIped wire-adhesive nail brace and the podofix active adhesive nail brace were applied. The COMBIped wire-adhesive nail brace consists of spring wire on one side and a plastic pad on the other, which is glued to the nail. The podofix active adhesive nail brace consists of an elastic plastic pad that is glued to the toe nail and tightened with a wire.
In the study by Erdogan & Erdogan in diabetics a nail brace with two hook like projections on the sides, and a dental string in the middle pulling the sides of the nail upwards was used.
3TO BRACE
In the study of children with ingrown toenails by Shih et al. three types of nail brace devices were used, namely a hook device (3TO-Brace, 3TO GmbH, Germany) in 5% of cases, an adhesive device (Podofix, 3TO GmbH, Germany) in 13% of cases or a composite device consisting of a wire and an adhesive pad (COMBIped, 3TO GmbH, Germany) in 76% of cases. Generally, hook devices and composite devices were considered more effective than adhesive devices by the authors of the study.
However, a hook device can only be applied when a nail fold is accessible. When none of the nail folds can be accessed or when a patient has extremely thin nails an adhesive device has to be used.
Cosmetic Adhesive Nail Braces
BS Adhesive Nail Brace
The BS adhesive nail brace is an extremely flat leaf spring made of high-performance plastic. Glued across the entire width of the big toenail, the spring forces are distributed over the whole curvature of the nail. Functionally, the BS nail brace corresponds to a leaf spring. By applying the flat brace to the curved, ingrown nail, it transfers its own restoring forces to the nail. The nail is gently lifted out of the nail fold. Pain is relieved within minutes after the application of the BS adhesive nail brace.
PODOSTRIPE Glue-on Nail Brace
The PODOSTRIPE Glue-on Nail Brace is a rubber band that is stretched when it is applied to the nail. The soft material of the PODOSTRIPE Glue-on Nail Brace can be used on all nail shapes and PODOSTRIPE Glue-on Nail Brace is suitable for the cosmetic correction of nearly all cases of deformed, ingrown and involuted nails. In addition PODOSTRIPE Glue-on Brace is suitable for diabetics and children. PODOSTRIPE Glue-on Brace can provide instant pain relief in the case of ingrown nails. The application is simple as shown in the video below.
As shown in the embedded video below a narrow band of UV nail gel is applied to the beginning of the nail. By curing the gel with LED blue light, the gel shrinks a little. The slightly shrunk gel holds the nail in its shape while the nail grows out. As a result, the screwed-in corners of the nail must inevitably „twist out“ over time.
Self-treatment of ingrown toenails with a nail brace
CurveCorrect Nail Brace
The CurveCorrect ingrown toenail brace is a thin, reinforced composite strip that is glued on the surface of the toenail. The CurveCorrect Nail Brace acts like a spring, gently straightening and lifting each side of the toenail, reducing its pressure against the skin in the nailfold. Correction occurs over a period of weeks.